

Tracking preventable deaths in December 2024
The prison crisis, ambulance delays and neonatal deaths - welcome to the last monthly review of 2024

December is a difficult month for many bereaved who enter the festive period without their loved ones. With the growing delays of inquests, some taking more than two years before there is a conclusion or a hearing, grief is prolonged - unnecessarily compounding harm.
The current pace of the ‘system’ reduces its ability to effectively “learn lessons” that can immediately prevent similar deaths - something a real-time centralised database can solve, disseminating lessons as soon as the information enters the system.
In December, the UK government announced plans to address prison overcrowding, with further warnings about the capacity of prisons. If you missed it, take a read of the PDT’s analysis of prison deaths reported by coroners - will more mechanisms really solve the problem?
Deaths in prison, who's tracking?

The UK is in the midst of a prison crisis. The prison population reached record highs, with the Government releasing thousands of prisoners early since September. Now, £2.3 billion has been allocated to build new prisons.
Since my analysis, two more coroners reports have been sent to prisons, including HM Prison Coldingley and Eastwood Park. Another coroner’s report was sent to HM Prison and Probation Service, bringing their total to at least 154 reports. In December, the first report to the Parole Board was also published. As the prison crisis continues, I predict we will see many more reports sent to these organisations.
On Thursday, 12 December 2024, I was invited to the House of Lords for the National State of Patient Safety Report launch event.

The work of the Preventable Deaths Tracker contributed to Part 3 of the report on using data to inform national patient safety priorities. However, the real achievement for the Preventable Deaths Tracker will be when the NHS actually starts using coroner data to prevent future deaths, nationally.
My highlight from the evening was speaking in person with the many patient safety champions that I’ve followed online for many years, including James Titcombe OBE, Dr Henrietta Hughes OBE, and the new Minister for Patient Safety, Women’s Health and Mental Health, Baroness Gillian Merron. A huge thank you to the Institute of Global Health Innovation at Imperial College London and Patient Safety Watch for extending the warm welcome and invitation.
Before I get onto the usual monthly analysis of coroner reports, I wanted to share two reports published in December that require highlighting. The first is another neonatal death, just 37 minutes after birth. The coroner raised many concerns regarding neglect in care, but notably, the Trust’s inability to appropriately review and refer deaths to the coroner - failing to comply with the duty of candour. This is the first time I’ve seen such a concern raised in a Prevention of Future Death report, and it’s also the first sent to the National Medical Examiner.
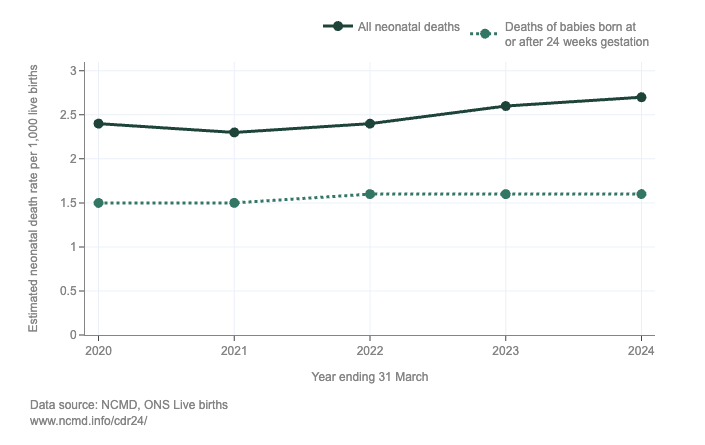
In England, all deaths in those under 18 must be reviewed, and learnings centralised in the National Child Mortality Database (NCMD). Over £3.5 million has been allocated to the University of Bristol for the NCMD by NHS England, with neonatal deaths increasing since records began. In 2021, NHS England set a neonatal mortality rate ambition of 1.0 deaths per 1,000 live births for 2025 - but trends are going in the opposite direction.
The second report describes yet another death following an 8.5-hour ambulance delay. Ambulance delays are now one of the most common concerns raised by coroners in reports. In this Prevention of Future Death report, the Senior Coroner refers to data from the Preventable Deaths Tracker and my recent analysis of reports sent to Ambulance Trusts to highlight the national problem and lack of oversight.

I am always thrilled to see how the Tracker is being used by those working hard to prevent future deaths. An ambulance delay should be a “never event”, not the norm. Now, onto the December statistics.
Keep reading with a 7-day free trial
Subscribe to Preventable Deaths Tracker to keep reading this post and get 7 days of free access to the full post archives.